A 13 minute read. Updated September 2026.
Eighteen months into playing padel four or five times a week, I started noticing something at my club. On any given evening, at least three or four players were wearing some kind of brace, tape, or compression sleeve. Elbow bands. Knee sleeves. Shoulder strapping. Ankle braces. Calf compression.
At first I thought I was just paying more attention because I was dealing with my own elbow problem. Then I started counting. Conservatively, on a typical Tuesday evening session with eight courts running, I'd see seven or eight obviously injured players. Out of maybe thirty two people total. That's a quarter of the room playing through some kind of physical issue.
This is normal for padel. It shouldn't be. Below is what's actually going on and how to stay off the brace list.
Why padel hurts more than people think
Padel looks like a low-impact, low-injury sport. Small court. Walls to bounce balls off. Lower running distance than tennis. Slower ball speeds. Less aggressive technique than squash.
The injury data tells a different story.
The 2023 systematic review in BMJ Open Sport and Exercise Medicine looked at injury rates across multiple racquet sports. Padel showed injury incidence rates comparable to recreational tennis, despite the apparent gentler profile. The lateral epicondyle (outside of the elbow) was the single most common injury location, but the spread across the body was wide.
Smith Palacio's 2024 study in Ciencia y Deporte broke down injury patterns specifically in amateur padel players. The conclusion: the sport's apparent simplicity masks specific biomechanical demands that produce predictable injuries when amateurs play with poor technique, inadequate equipment, or insufficient conditioning.
Three things about padel produce most injuries.
First, the pala has no strings. Vibration from impact transfers directly to the arm. I covered this in detail in my separate article on padel elbow.
Second, the court has walls that change the rhythm of the game. Sudden direction changes, planting steps to reverse momentum, lunges into corners. These movements load the knee, ankle, and hip in ways most amateurs aren't conditioned for.
Third, the social culture of the sport. People play with friends regardless of fitness level, often after sedentary work weeks, frequently into their forties, fifties, and sixties. The bodies playing the sport are not, on average, prepared for the demands the sport places on them.
Add these together and you get the locker room of braces.
The injury data tells a different story.
The 2023 systematic review in BMJ Open Sport and Exercise Medicine looked at injury rates across multiple racquet sports. Padel showed injury incidence rates comparable to recreational tennis, despite the apparent gentler profile. The lateral epicondyle (outside of the elbow) was the single most common injury location, but the spread across the body was wide.
Smith Palacio's 2024 study in Ciencia y Deporte broke down injury patterns specifically in amateur padel players. The conclusion: the sport's apparent simplicity masks specific biomechanical demands that produce predictable injuries when amateurs play with poor technique, inadequate equipment, or insufficient conditioning.
Three things about padel produce most injuries.
First, the pala has no strings. Vibration from impact transfers directly to the arm. I covered this in detail in my separate article on padel elbow.
Second, the court has walls that change the rhythm of the game. Sudden direction changes, planting steps to reverse momentum, lunges into corners. These movements load the knee, ankle, and hip in ways most amateurs aren't conditioned for.
Third, the social culture of the sport. People play with friends regardless of fitness level, often after sedentary work weeks, frequently into their forties, fifties, and sixties. The bodies playing the sport are not, on average, prepared for the demands the sport places on them.
Add these together and you get the locker room of braces.
The 7 most common padel injuries, in rough order of frequency
Based on the BMJ systematic review, Smith Palacio's amateur data, and what I see at my own club, here are the injuries you'll actually encounter. None of this is a substitute for seeing a physiotherapist if you're already hurt.
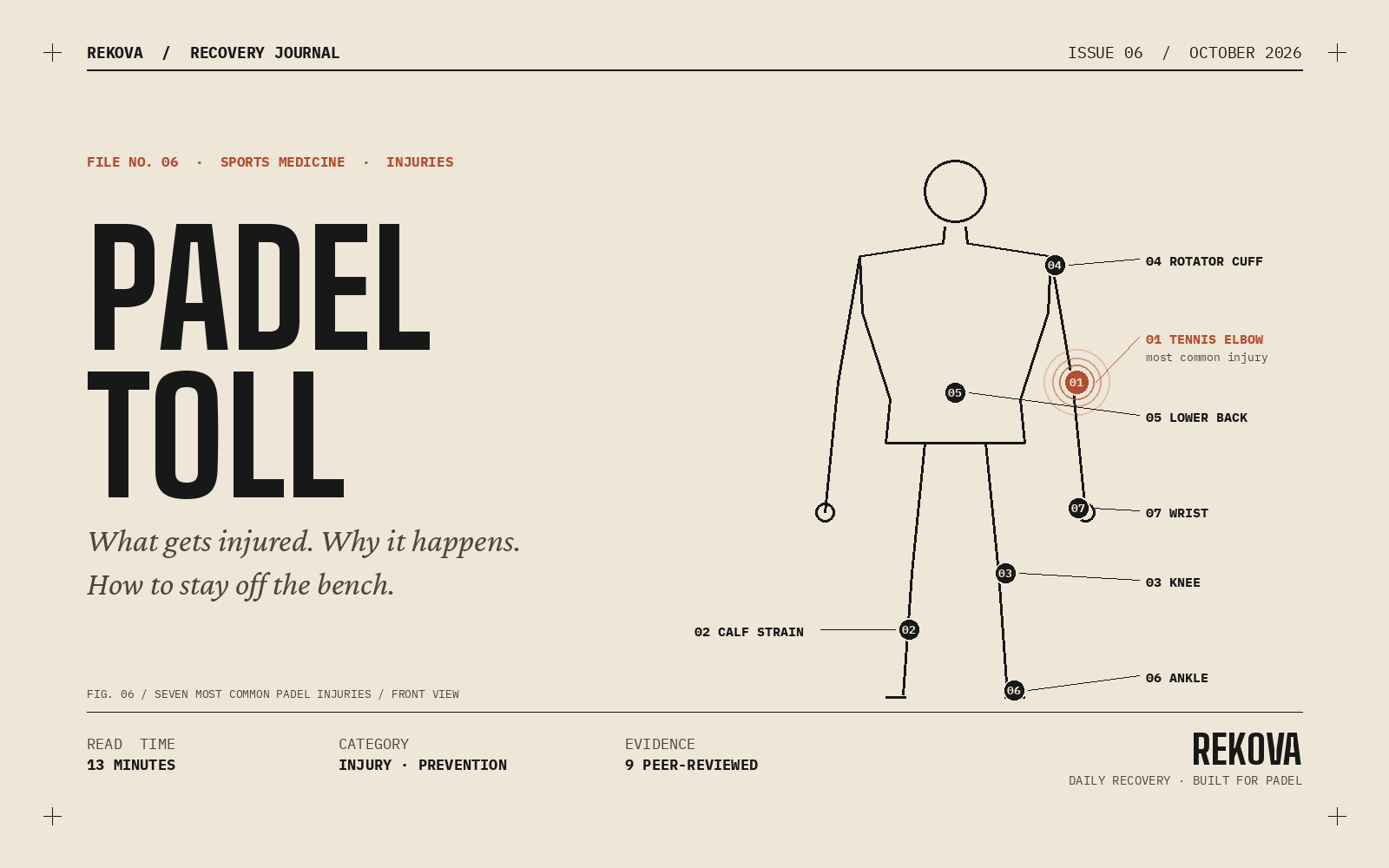
The list, in order:
Tennis elbow (lateral epicondylitis)
Calf strain or partial tear, sometimes called tennis leg
Knee injuries (patellar tendinopathy, meniscus, ligament strains)
Rotator cuff issues in the shoulder
Lower back pain
Ankle sprains
Wrist and hand injuries
Below I'll go through each one with what to watch for, what causes it, and basic prevention.
The list, in order:
Tennis elbow (lateral epicondylitis)
Calf strain or partial tear, sometimes called tennis leg
Knee injuries (patellar tendinopathy, meniscus, ligament strains)
Rotator cuff issues in the shoulder
Lower back pain
Ankle sprains
Wrist and hand injuries
Below I'll go through each one with what to watch for, what causes it, and basic prevention.
Tennis elbow (lateral epicondylitis)
The number one injury in padel by a wide margin. Already covered in my dedicated article on padel elbow. Quick version here.
Pain on the outside of the elbow, gradually building over weeks. Weak grip when lifting one-handed. Stiffness in the morning. Occasional sharp pain when extending the arm under load.
Causes. The stringless pala. Backhand technique, especially one-handed backhands. Too much playing volume too soon. Wrong grip size. Tight grip throughout the match instead of just at impact.
Prevention. Right pala for your body, under 350 grams for most amateurs. Two-handed backhand if the one-handed version gives you trouble. Loose grip between shots. Build playing volume gradually. Stretch forearms before and after matches.
Treatment. Rest the first week. Then progressive eccentric loading exercises. Counter-force brace during rehabilitation. Full return at six to eight weeks with proper protocol.
Pain on the outside of the elbow, gradually building over weeks. Weak grip when lifting one-handed. Stiffness in the morning. Occasional sharp pain when extending the arm under load.
Causes. The stringless pala. Backhand technique, especially one-handed backhands. Too much playing volume too soon. Wrong grip size. Tight grip throughout the match instead of just at impact.
Prevention. Right pala for your body, under 350 grams for most amateurs. Two-handed backhand if the one-handed version gives you trouble. Loose grip between shots. Build playing volume gradually. Stretch forearms before and after matches.
Treatment. Rest the first week. Then progressive eccentric loading exercises. Counter-force brace during rehabilitation. Full return at six to eight weeks with proper protocol.
Calf strain or tennis leg
This is one of the more dramatic injuries. Players describe it as feeling like they were shot in the calf. Sudden sharp pain, sometimes a popping sensation, immediate inability to bear weight on the leg.
The Bandeja Shop clinical guide describes it as particularly common in men aged 35 to 55 who are active but not specifically conditioned for explosive movement. That's most amateur padel players, especially the ones who picked up the sport in middle age.
The mechanism is typically a sudden push-off from the back foot to move forward to the net, or a planted lateral step to reverse direction. The medial gastrocnemius (the inner part of the calf muscle) takes most of the load and can partially tear.
Signs. Sudden pain, swelling, bruising that often spreads down to the ankle within a day. Difficulty walking. Visible deformity in severe cases.
Prevention. Proper warmup with dynamic calf work. Avoid playing on cold legs. Build calf strength with single-leg raises in your weekly routine. Don't try to play full intensity after long periods of inactivity without ramping up gradually.
Treatment. Initial rest, ice, compression, elevation for 48 to 72 hours. See a physiotherapist for proper grading. Recovery ranges from 2 weeks for mild cases to 8 weeks for significant tears. Returning too early is the most common reason people retear.
The Bandeja Shop clinical guide describes it as particularly common in men aged 35 to 55 who are active but not specifically conditioned for explosive movement. That's most amateur padel players, especially the ones who picked up the sport in middle age.
The mechanism is typically a sudden push-off from the back foot to move forward to the net, or a planted lateral step to reverse direction. The medial gastrocnemius (the inner part of the calf muscle) takes most of the load and can partially tear.
Signs. Sudden pain, swelling, bruising that often spreads down to the ankle within a day. Difficulty walking. Visible deformity in severe cases.
Prevention. Proper warmup with dynamic calf work. Avoid playing on cold legs. Build calf strength with single-leg raises in your weekly routine. Don't try to play full intensity after long periods of inactivity without ramping up gradually.
Treatment. Initial rest, ice, compression, elevation for 48 to 72 hours. See a physiotherapist for proper grading. Recovery ranges from 2 weeks for mild cases to 8 weeks for significant tears. Returning too early is the most common reason people retear.
Knee injuries
Two flavors. Chronic and acute.
Chronic knee issues in padel are usually patellar tendinopathy, sometimes called jumper's knee. Pain just below the kneecap. Builds slowly. Aggravated by sustained match play, especially anything involving deep lunges or repeated jumping for smashes.
Acute knee injuries include meniscus tears and ligament strains (medial collateral, lateral collateral, occasionally anterior cruciate). These happen during sudden direction changes, especially when the foot is planted and the body twists. The classic mechanism is chasing a ball wide, planting hard, then trying to push back to center while the knee is loaded.
ACL injuries deserve special mention. Female athletes have approximately 8 times higher rates of ACL injury than male athletes across most sports. The mechanisms in padel are exactly the type that produce these tears. Lateral lunges, planted twists, deceleration with rotation.
Prevention. Strength training the legs is non-negotiable if you play multiple times a week. Specifically single-leg work, lateral movements, eccentric strength of the quadriceps and hamstrings. Don't play through small knee pain that lasts more than a few days.
Treatment. Depends entirely on the diagnosis. See a sports doctor or orthopedist if you have acute knee pain, swelling, or instability. Don't self-diagnose serious knee injuries.
Chronic knee issues in padel are usually patellar tendinopathy, sometimes called jumper's knee. Pain just below the kneecap. Builds slowly. Aggravated by sustained match play, especially anything involving deep lunges or repeated jumping for smashes.
Acute knee injuries include meniscus tears and ligament strains (medial collateral, lateral collateral, occasionally anterior cruciate). These happen during sudden direction changes, especially when the foot is planted and the body twists. The classic mechanism is chasing a ball wide, planting hard, then trying to push back to center while the knee is loaded.
ACL injuries deserve special mention. Female athletes have approximately 8 times higher rates of ACL injury than male athletes across most sports. The mechanisms in padel are exactly the type that produce these tears. Lateral lunges, planted twists, deceleration with rotation.
Prevention. Strength training the legs is non-negotiable if you play multiple times a week. Specifically single-leg work, lateral movements, eccentric strength of the quadriceps and hamstrings. Don't play through small knee pain that lasts more than a few days.
Treatment. Depends entirely on the diagnosis. See a sports doctor or orthopedist if you have acute knee pain, swelling, or instability. Don't self-diagnose serious knee injuries.
Rotator cuff issues
The shoulder is small. The forces on it during a smash are large. The math eventually catches up.
The Padel Magazine guide and the Padel39 injury article both flag rotator cuff issues as the third or fourth most common chronic problem in active players. Symptoms include pain at the front or side of the shoulder, weakness when raising the arm overhead, and difficulty sleeping on the affected side.
Causes. Repeated overhead motions with poor technique. Imbalance between internal and external rotators (most amateurs have stronger internal rotators from chest exercises and weaker external rotators from neglecting the back side). Inadequate warmup of the shoulder before play.
Prevention. External rotation strengthening exercises with a light band or cable. Foam rolling the chest and front shoulder. Proper smash technique that uses the whole kinetic chain (legs to hips to torso to arm), not just the arm.
Treatment. Rest from overhead motions. Physiotherapy with specific rotator cuff strengthening. Full return often takes longer than people expect. Six to twelve weeks is normal for a proper rehabilitation.
The Padel Magazine guide and the Padel39 injury article both flag rotator cuff issues as the third or fourth most common chronic problem in active players. Symptoms include pain at the front or side of the shoulder, weakness when raising the arm overhead, and difficulty sleeping on the affected side.
Causes. Repeated overhead motions with poor technique. Imbalance between internal and external rotators (most amateurs have stronger internal rotators from chest exercises and weaker external rotators from neglecting the back side). Inadequate warmup of the shoulder before play.
Prevention. External rotation strengthening exercises with a light band or cable. Foam rolling the chest and front shoulder. Proper smash technique that uses the whole kinetic chain (legs to hips to torso to arm), not just the arm.
Treatment. Rest from overhead motions. Physiotherapy with specific rotator cuff strengthening. Full return often takes longer than people expect. Six to twelve weeks is normal for a proper rehabilitation.
Lower back pain
This one is partly the sport and partly the modern life that surrounds the sport.
Padel involves repeated rotation of the trunk on most shots. The lower spine handles those rotational forces. If the supporting muscles (core, glutes, hip flexors) are weak from sedentary work, the spine takes more of the load than it should.
Add lunges into corners, sudden hip flexion to chase low balls, and the occasional awkward extension to reach high lobs. You get a recipe for chronic low-back tightness in players who don't do complementary strength work.
Signs. Aching in the lower back during or after matches. Stiffness in the morning, especially on Mondays after weekend play. Occasional sharp twinges during specific movements like getting out of the car.
Prevention. Core strengthening (planks, dead bugs, bird dogs). Hip mobility work. Glute strengthening, especially the medius and minimus that stabilize the pelvis. Reduce overall sedentary time during the work week. Take micro-breaks during long desk sessions.
Treatment. If acute and severe, see a physiotherapist. For chronic mild tightness, daily mobility work and strengthening usually helps within weeks.
Padel involves repeated rotation of the trunk on most shots. The lower spine handles those rotational forces. If the supporting muscles (core, glutes, hip flexors) are weak from sedentary work, the spine takes more of the load than it should.
Add lunges into corners, sudden hip flexion to chase low balls, and the occasional awkward extension to reach high lobs. You get a recipe for chronic low-back tightness in players who don't do complementary strength work.
Signs. Aching in the lower back during or after matches. Stiffness in the morning, especially on Mondays after weekend play. Occasional sharp twinges during specific movements like getting out of the car.
Prevention. Core strengthening (planks, dead bugs, bird dogs). Hip mobility work. Glute strengthening, especially the medius and minimus that stabilize the pelvis. Reduce overall sedentary time during the work week. Take micro-breaks during long desk sessions.
Treatment. If acute and severe, see a physiotherapist. For chronic mild tightness, daily mobility work and strengthening usually helps within weeks.
Ankle sprains
The classic acute injury. One bad step and you're out for two to six weeks.
Mechanism is almost always the same. Sudden change of direction, foot lands at an awkward angle, the ankle rolls. Sometimes happens chasing a wide ball at the net. Sometimes happens just stepping back to set up for a smash.
The 2024 Smith Palacio study noted that female players had higher adoption of padel-specific shoes (41.6% versus 18.7% in men). Counterintuitively, the men playing in tennis or running shoes were having more ankle issues. The right shoes matter for this sport.
Prevention. Padel-specific shoes are not just marketing. They have a wider base, better lateral support, and grip suited to artificial turf. Worth the money. Ankle strengthening through balance work and proprioception training (single-leg stands, wobble boards).
Treatment. Initial rest, ice, compression, elevation. See a physiotherapist for grading. Most ankle sprains return to play within 2 to 6 weeks depending on severity. Continue strength training of the ankle for at least 3 months after to prevent recurrence. Ankle sprains are notorious for coming back if you don't rehabilitate fully.
Mechanism is almost always the same. Sudden change of direction, foot lands at an awkward angle, the ankle rolls. Sometimes happens chasing a wide ball at the net. Sometimes happens just stepping back to set up for a smash.
The 2024 Smith Palacio study noted that female players had higher adoption of padel-specific shoes (41.6% versus 18.7% in men). Counterintuitively, the men playing in tennis or running shoes were having more ankle issues. The right shoes matter for this sport.
Prevention. Padel-specific shoes are not just marketing. They have a wider base, better lateral support, and grip suited to artificial turf. Worth the money. Ankle strengthening through balance work and proprioception training (single-leg stands, wobble boards).
Treatment. Initial rest, ice, compression, elevation. See a physiotherapist for grading. Most ankle sprains return to play within 2 to 6 weeks depending on severity. Continue strength training of the ankle for at least 3 months after to prevent recurrence. Ankle sprains are notorious for coming back if you don't rehabilitate fully.
Wrist and hand injuries
The smallest of the common issues but worth covering.
Pain at the base of the thumb, on the back of the wrist, or in the forearm near the wrist. Usually develops from gripping the pala too tightly, from impact angles that load the wrist wrong, or from falls.
The Padel39 article covers this in their general injury overview. Wrist tendonitis specifically is the variant most players see, often from holding a too-thin grip that requires harder squeezing to control.
Prevention. Grip size matters (L2 or L3 for most players). Relax the grip between shots. Use proper impact technique. Avoid the muscle memory from tennis if you came from that sport. Tennis grips are different.
Treatment. Rest, ice for acute pain. Forearm and wrist stretching. If pain persists past two weeks, see a hand specialist or sports physiotherapist.
Pain at the base of the thumb, on the back of the wrist, or in the forearm near the wrist. Usually develops from gripping the pala too tightly, from impact angles that load the wrist wrong, or from falls.
The Padel39 article covers this in their general injury overview. Wrist tendonitis specifically is the variant most players see, often from holding a too-thin grip that requires harder squeezing to control.
Prevention. Grip size matters (L2 or L3 for most players). Relax the grip between shots. Use proper impact technique. Avoid the muscle memory from tennis if you came from that sport. Tennis grips are different.
Treatment. Rest, ice for acute pain. Forearm and wrist stretching. If pain persists past two weeks, see a hand specialist or sports physiotherapist.
Men versus women: different injury patterns
The 2024 Smith Palacio paper found gender-specific patterns worth understanding.
Women showed higher rates of lower extremity injuries overall, ligament sprains specifically, ACL injuries in particular (the 8x cross-sport pattern shows up in padel too), and wrist injuries from grip and impact issues.
Men showed higher rates of muscle strains particularly calf tears, lower back pain, shoulder injuries from aggressive smash technique, and tendon overuse injuries including tennis elbow.
The total injury rate was similar between sexes. The distribution differed. This matters for prevention strategy. Women should prioritize lower-body strength, ankle stability, and core work. Men should prioritize mobility, posterior chain strength, and not playing through small muscle issues.
Worth noting briefly. Hormonal factors influence connective tissue laxity through the menstrual cycle. Research suggests injury risk varies on specific cycle days. The data is emerging but the pattern is real. Not something most amateurs need to track day by day, but worth being aware of.
Women showed higher rates of lower extremity injuries overall, ligament sprains specifically, ACL injuries in particular (the 8x cross-sport pattern shows up in padel too), and wrist injuries from grip and impact issues.
Men showed higher rates of muscle strains particularly calf tears, lower back pain, shoulder injuries from aggressive smash technique, and tendon overuse injuries including tennis elbow.
The total injury rate was similar between sexes. The distribution differed. This matters for prevention strategy. Women should prioritize lower-body strength, ankle stability, and core work. Men should prioritize mobility, posterior chain strength, and not playing through small muscle issues.
Worth noting briefly. Hormonal factors influence connective tissue laxity through the menstrual cycle. Research suggests injury risk varies on specific cycle days. The data is emerging but the pattern is real. Not something most amateurs need to track day by day, but worth being aware of.
Age and injury risk
Older players don't necessarily get more injuries. They get different injuries and recover slower from them.
Tendon issues become more common after 35 to 40. The tissue is less elastic and slower to remodel. This is why padel elbow is more common in middle-aged amateurs than in young players.
Muscle injuries also shift with age. The calf strain that happens to a 50 year old player is rarely the same severity that happens to a 25 year old. Older tissue tears more easily and heals slower.
Joint issues accumulate. The wear on a 55 year old knee with 30 years of various sports behind it is different from a 25 year old knee.
The good news. Most age-related injury risk responds to consistent strength training, proper warmup, and respect for recovery. The same things that work for younger players, just applied more strictly.
Tendon issues become more common after 35 to 40. The tissue is less elastic and slower to remodel. This is why padel elbow is more common in middle-aged amateurs than in young players.
Muscle injuries also shift with age. The calf strain that happens to a 50 year old player is rarely the same severity that happens to a 25 year old. Older tissue tears more easily and heals slower.
Joint issues accumulate. The wear on a 55 year old knee with 30 years of various sports behind it is different from a 25 year old knee.
The good news. Most age-related injury risk responds to consistent strength training, proper warmup, and respect for recovery. The same things that work for younger players, just applied more strictly.
What actually prevents most padel injuries
Strip away the noise. Here is what consistently shows up across research and across actual physiotherapy practice as the highest-impact prevention.
Strength training. Twice a week, focused on legs, core, and posterior chain. Single leg work especially. This addresses 60 to 70 percent of injury risk by itself. Most amateurs play padel as their only physical activity. That's a setup for problems.
Proper warmup. Minimum 10 minutes of dynamic mobility before playing hard. Calf raises, leg swings, arm circles, light rallies. Cold tendons and muscles are vulnerable tendons and muscles.
Equipment that fits you. Right pala weight and shape. Right grip size. Padel-specific shoes. Stop trying to play in tennis shoes because they're cheaper.
Volume management. Two consecutive hard sessions before a rest or easy day. Don't go from one session a week to five sessions a week in a month. Build gradually.
Recovery between sessions. Sleep, nutrition, hydration. I covered each of these in separate articles on padel recovery and padel nutrition. They matter as much for injury prevention as they do for performance.
Address small issues immediately. The little twinge in your knee that's been there for two weeks is giving you information. Listen. Take a few days off, do mobility work, address the cause. Don't keep playing on it for three months until it becomes a real injury.
Nutritional foundation. Adequate protein for tissue repair. Adequate calcium and magnesium for muscle function. Vitamin C and collagen for connective tissue. Most amateurs run low on at least one of these.
Strength training. Twice a week, focused on legs, core, and posterior chain. Single leg work especially. This addresses 60 to 70 percent of injury risk by itself. Most amateurs play padel as their only physical activity. That's a setup for problems.
Proper warmup. Minimum 10 minutes of dynamic mobility before playing hard. Calf raises, leg swings, arm circles, light rallies. Cold tendons and muscles are vulnerable tendons and muscles.
Equipment that fits you. Right pala weight and shape. Right grip size. Padel-specific shoes. Stop trying to play in tennis shoes because they're cheaper.
Volume management. Two consecutive hard sessions before a rest or easy day. Don't go from one session a week to five sessions a week in a month. Build gradually.
Recovery between sessions. Sleep, nutrition, hydration. I covered each of these in separate articles on padel recovery and padel nutrition. They matter as much for injury prevention as they do for performance.
Address small issues immediately. The little twinge in your knee that's been there for two weeks is giving you information. Listen. Take a few days off, do mobility work, address the cause. Don't keep playing on it for three months until it becomes a real injury.
Nutritional foundation. Adequate protein for tissue repair. Adequate calcium and magnesium for muscle function. Vitamin C and collagen for connective tissue. Most amateurs run low on at least one of these.
Where supplements and nutrition fit
For injury prevention specifically, micronutrient adequacy matters. The EFSA-approved health claims that are directly relevant: magnesium contributes to normal muscle function, vitamin C contributes to normal collagen formation for the normal function of cartilage and bones, calcium contributes to normal muscle function, vitamin D contributes to normal absorption of calcium and to the normal function of muscles.
These are not optional nutrients if you're playing several times a week. They're foundational for the tissues that take the load.
Hydrolyzed collagen has emerging research support for connective tissue maintenance under athletic load. Not definitive yet. Worth watching the research as it develops.
This is the gap a daily recovery drink fills if your regular diet has gaps, which most realistic adult diets do. The Rekova formula was designed around exactly this profile. Electrolytes for what you sweat out. Magnesium and B vitamins for muscle and energy support. Hydrolyzed collagen with vitamin C for connective tissue. CoQ10 and Acetyl-L-Carnitine for cellular support. Adaptogens and antioxidants on top.
Not a treatment for injuries. Nutritional support for the body that has to keep performing.
These are not optional nutrients if you're playing several times a week. They're foundational for the tissues that take the load.
Hydrolyzed collagen has emerging research support for connective tissue maintenance under athletic load. Not definitive yet. Worth watching the research as it develops.
This is the gap a daily recovery drink fills if your regular diet has gaps, which most realistic adult diets do. The Rekova formula was designed around exactly this profile. Electrolytes for what you sweat out. Magnesium and B vitamins for muscle and energy support. Hydrolyzed collagen with vitamin C for connective tissue. CoQ10 and Acetyl-L-Carnitine for cellular support. Adaptogens and antioxidants on top.
Not a treatment for injuries. Nutritional support for the body that has to keep performing.
FAQ: questions about padel injuries
How common are padel injuries really? Estimates from the BMJ 2023 systematic review put incidence at around 3 to 7 injuries per 1000 hours of play for amateurs. Higher than most people expect for what looks like a gentle sport.
Should I see a doctor or wait? Sharp acute pain after a specific incident means see someone. Mild lingering soreness that improves with rest can wait a week or two before professional input. Pain that's getting worse despite rest needs professional evaluation soon.
Can I play through a minor injury? Sometimes. Depends on the type. Mild muscle soreness, yes. Tendon pain that's stable, sometimes, with caution. Acute joint pain, sharp pains, or anything getting worse, no.
What's the most preventable injury? Tennis elbow. The right pala, right grip, right technique, and gradual volume increase prevent the vast majority of cases.
What's the least preventable injury? Acute ankle sprains. Padel-specific shoes help. Ankle strengthening helps. But sometimes you step wrong and that's that.
Should I use compression sleeves preventively? For specific injuries during rehabilitation, yes. As preventive gear for healthy players, the evidence is weak. Don't rely on a sleeve to fix bad technique or insufficient strength.
Will I get injured if I play three or four times a week? Eventually most heavy amateurs experience something. The question is whether it's a small lesson learned or a chronic problem you play through. Good habits keep it as the first kind.
How long should I rest after an injury before returning? Depends on the type and severity. The general principle is that you should be completely pain-free during normal activities for at least a few days before testing it on the court. Returning to pain is the fastest way to make an injury chronic.
Are some clubs or surfaces worse for injuries? Outdoor courts with weather variation, older artificial grass that's lost its grip, and very hot indoor conditions all increase injury risk. Better facilities matter more than people think.
Should I see a doctor or wait? Sharp acute pain after a specific incident means see someone. Mild lingering soreness that improves with rest can wait a week or two before professional input. Pain that's getting worse despite rest needs professional evaluation soon.
Can I play through a minor injury? Sometimes. Depends on the type. Mild muscle soreness, yes. Tendon pain that's stable, sometimes, with caution. Acute joint pain, sharp pains, or anything getting worse, no.
What's the most preventable injury? Tennis elbow. The right pala, right grip, right technique, and gradual volume increase prevent the vast majority of cases.
What's the least preventable injury? Acute ankle sprains. Padel-specific shoes help. Ankle strengthening helps. But sometimes you step wrong and that's that.
Should I use compression sleeves preventively? For specific injuries during rehabilitation, yes. As preventive gear for healthy players, the evidence is weak. Don't rely on a sleeve to fix bad technique or insufficient strength.
Will I get injured if I play three or four times a week? Eventually most heavy amateurs experience something. The question is whether it's a small lesson learned or a chronic problem you play through. Good habits keep it as the first kind.
How long should I rest after an injury before returning? Depends on the type and severity. The general principle is that you should be completely pain-free during normal activities for at least a few days before testing it on the court. Returning to pain is the fastest way to make an injury chronic.
Are some clubs or surfaces worse for injuries? Outdoor courts with weather variation, older artificial grass that's lost its grip, and very hot indoor conditions all increase injury risk. Better facilities matter more than people think.
The short version
Padel produces more injuries than its gentle reputation suggests. Seven common injuries account for most of what you'll see at any club. Elbow, calf, knee, shoulder, lower back, ankle, wrist. The common factor is that most are preventable through strength training, proper warmup, right equipment, gradual volume increase, and respect for recovery. Address small issues fast before they become big ones. The boring fundamentals work for injury prevention as much as they work for performance.
If you're already injured, see a physiotherapist. No article replaces a real diagnosis and rehabilitation plan.
If you're already injured, see a physiotherapist. No article replaces a real diagnosis and rehabilitation plan.
Sources
Dahmen J. et al. Incidence, prevalence and nature of injuries in padel: a systematic review. BMJ Open Sport and Exercise Medicine. 2023.
Smith Palacio E. Epidemiologia de las lesiones en padel y recomendaciones preventivas. Ciencia y Deporte. April 2024.
Isokinetic Medical Group. The Padel Player's Elbow: How to Prevent and Treat It. February 2025.
Corcuera Padel Club. Understanding Tennis Elbow in Padel. 2025.
Padel39. The Most Common Padel Injuries and How to Prevent Them. 2026.
Padel Magazine. How to Avoid the Padel Elbow. 2020.
Bandeja Shop. Common Padel Injuries and Recovery Approaches. 2025.
Padel Rumors. 7 Padel-Specific Muscle Recovery Tips for 2025. July 2025.
EFSA. Scientific Opinions on the substantiation of health claims related to magnesium, vitamin C, calcium, vitamin D, and collagen. EFSA Journal, various years.
This article reflects current research on padel injuries and my own experience playing and watching teammates over years at the club. It is not medical advice. If you have any of the symptoms or injuries described here, please consult a qualified healthcare professional. No article can replace proper diagnosis and a personalized rehabilitation plan.
Rekova does not treat injuries and is not a substitute for medical care. It is a daily functional drink with electrolytes, magnesium, hydrolyzed collagen, B vitamins, vitamin C, and supporting nutrients, formulated as nutritional support for people who play padel regularly.
Smith Palacio E. Epidemiologia de las lesiones en padel y recomendaciones preventivas. Ciencia y Deporte. April 2024.
Isokinetic Medical Group. The Padel Player's Elbow: How to Prevent and Treat It. February 2025.
Corcuera Padel Club. Understanding Tennis Elbow in Padel. 2025.
Padel39. The Most Common Padel Injuries and How to Prevent Them. 2026.
Padel Magazine. How to Avoid the Padel Elbow. 2020.
Bandeja Shop. Common Padel Injuries and Recovery Approaches. 2025.
Padel Rumors. 7 Padel-Specific Muscle Recovery Tips for 2025. July 2025.
EFSA. Scientific Opinions on the substantiation of health claims related to magnesium, vitamin C, calcium, vitamin D, and collagen. EFSA Journal, various years.
This article reflects current research on padel injuries and my own experience playing and watching teammates over years at the club. It is not medical advice. If you have any of the symptoms or injuries described here, please consult a qualified healthcare professional. No article can replace proper diagnosis and a personalized rehabilitation plan.
Rekova does not treat injuries and is not a substitute for medical care. It is a daily functional drink with electrolytes, magnesium, hydrolyzed collagen, B vitamins, vitamin C, and supporting nutrients, formulated as nutritional support for people who play padel regularly.
