A 13 minute read. Updated December 2026.
There's a player at my club called Patricia. She's 41, works in product management at a software company in Madrid, has been playing padel for about six years. She's roughly my level, which means we sometimes play mixed doubles when both our regular partners cancel.
About a year ago I asked her, casually, why she'd switched her training routine. She'd suddenly been spending more time on specific knee strengthening exercises and changed her electrolyte product. She paused for a second, then said something simple. Nobody is writing this stuff for women, she said. So she had to learn it herself.
I spent the next few months talking to her and a couple of other female players at the club. Reading the research on female athletes that exists. Looking at what's specific to padel and what's general to all women's sports.
I want to be upfront. I am not a woman. I am not a doctor. What I'm sharing here is research-based observations and what I've learned from female players I respect, framed for women who play padel and want to understand what's actually different and what's just marketing.
Below is what I've put together.
Why this article exists
Most padel research uses male subjects. The general sports science literature historically has a roughly 6 to 1 male-to-female ratio in study subjects. Recent years have improved this somewhat but the gap is still significant.
The result is that nearly everything written about training, recovery, and nutrition for sport tacitly assumes male physiology as the default. Women players have to either trust that those recommendations apply unchanged or do their own research to figure out what's different.
For padel specifically, the gap is wider. The sport is newer. The research base is thinner. And women's participation has grown rapidly only in the last few years.
So here's what's actually known. The honest version.
The result is that nearly everything written about training, recovery, and nutrition for sport tacitly assumes male physiology as the default. Women players have to either trust that those recommendations apply unchanged or do their own research to figure out what's different.
For padel specifically, the gap is wider. The sport is newer. The research base is thinner. And women's participation has grown rapidly only in the last few years.
So here's what's actually known. The honest version.
Where the real differences are (and where they aren't)
Most of what works for performance is the same regardless of sex. Sleep, nutrition, training, recovery, mental preparation. The fundamentals are not sex-specific.
But there are several areas where biology genuinely differs in ways that matter for padel.
Body composition. Women on average have higher body fat percentages and lower muscle mass relative to body weight. This affects energy metabolism, power-to-weight ratio, and thermoregulation during play.
Joint structure. Women typically have wider pelvises which changes the Q-angle of the knee joint. This relates to higher ACL injury risk that I'll cover below.
Hormonal cycles. Menstrual cycles cause systematic variations in joint laxity, energy availability, body temperature regulation, and recovery capacity. These aren't dramatic but they're real.
Iron metabolism. Menstruating women lose iron monthly that men don't. Iron deficiency is significantly more common in women athletes.
Bone density trajectory. After menopause, women face a steeper bone density decline than age-matched men experience.
Pregnancy and postpartum. The most obvious women-specific situation, with multiple distinct phases that affect what's possible and what's safe.
These are the categories where the conversation needs to be specific. The rest mostly isn't.
But there are several areas where biology genuinely differs in ways that matter for padel.
Body composition. Women on average have higher body fat percentages and lower muscle mass relative to body weight. This affects energy metabolism, power-to-weight ratio, and thermoregulation during play.
Joint structure. Women typically have wider pelvises which changes the Q-angle of the knee joint. This relates to higher ACL injury risk that I'll cover below.
Hormonal cycles. Menstrual cycles cause systematic variations in joint laxity, energy availability, body temperature regulation, and recovery capacity. These aren't dramatic but they're real.
Iron metabolism. Menstruating women lose iron monthly that men don't. Iron deficiency is significantly more common in women athletes.
Bone density trajectory. After menopause, women face a steeper bone density decline than age-matched men experience.
Pregnancy and postpartum. The most obvious women-specific situation, with multiple distinct phases that affect what's possible and what's safe.
These are the categories where the conversation needs to be specific. The rest mostly isn't.
Injury patterns: what the data actually shows
I covered injuries in my separate article on padel injuries. The Smith Palacio 2024 study in Ciencia y Deporte was the most detailed look at gender-specific patterns in amateur padel.
Women showed higher rates of lower extremity ligament injuries, particularly knee and ankle. ACL tears specifically run about 8 times higher than men across most sports, and padel follows this pattern. Wrist injuries from grip and impact issues also appear more often in women players.
Men showed higher rates of muscle strains particularly calf tears, tendon overuse injuries including tennis elbow, lower back pain, and shoulder injuries from aggressive smash technique.
The total injury rate was similar. The pattern differed.
The implication for women players. Lower body strength training should be a priority. Knee stability exercises in particular. Single-leg work for ankle and knee proprioception. The specific drills your physiotherapist would recommend for ACL prevention work for padel just as well as they do for other sports.
The 41.6 percent versus 18.7 percent statistic from Smith Palacio about padel-specific shoe adoption is interesting. Women players are far more likely to invest in proper footwear. Good. Keep doing that. The men should catch up.
Women showed higher rates of lower extremity ligament injuries, particularly knee and ankle. ACL tears specifically run about 8 times higher than men across most sports, and padel follows this pattern. Wrist injuries from grip and impact issues also appear more often in women players.
Men showed higher rates of muscle strains particularly calf tears, tendon overuse injuries including tennis elbow, lower back pain, and shoulder injuries from aggressive smash technique.
The total injury rate was similar. The pattern differed.
The implication for women players. Lower body strength training should be a priority. Knee stability exercises in particular. Single-leg work for ankle and knee proprioception. The specific drills your physiotherapist would recommend for ACL prevention work for padel just as well as they do for other sports.
The 41.6 percent versus 18.7 percent statistic from Smith Palacio about padel-specific shoe adoption is interesting. Women players are far more likely to invest in proper footwear. Good. Keep doing that. The men should catch up.
The menstrual cycle and padel performance
Here's where the conversation gets specific and where research is still developing.
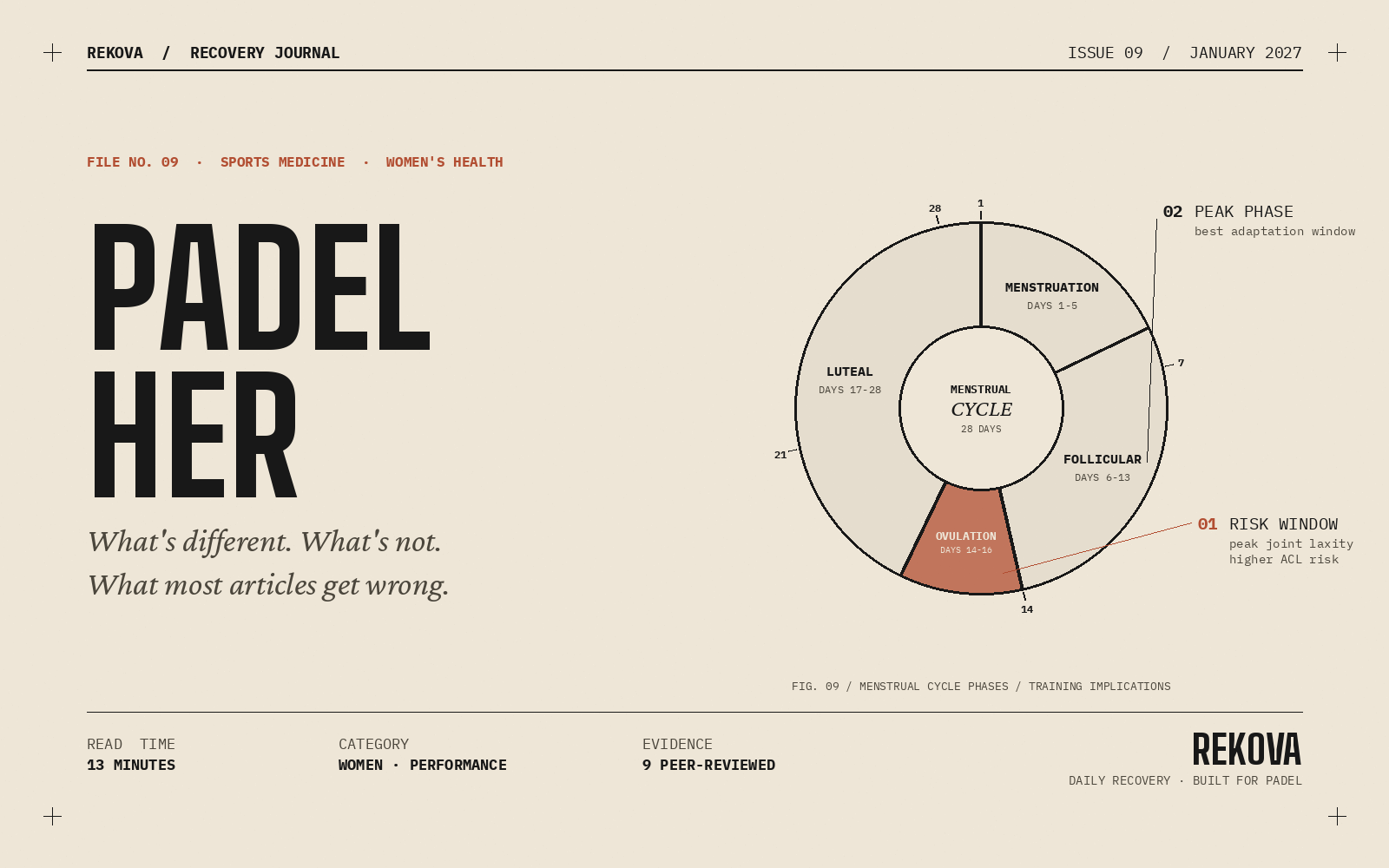
The menstrual cycle has four rough phases. Each phase has different hormonal profiles that affect physiological function.
Follicular phase, roughly days 1 to 14. Estrogen rises gradually. Most research suggests this is when training adaptations happen most effectively. Energy levels and motivation tend to be higher in the mid-to-late follicular phase. Many female athletes report feeling strongest in this window.
Ovulation, around day 14. Peak estrogen. Joint laxity is highest. This is one of the higher-risk windows for ligament injuries. Some research suggests reducing maximum-intensity work around ovulation to reduce ACL risk.
Luteal phase, days 15 to 28. Progesterone rises. Core body temperature increases slightly. Some women experience reduced cardiovascular efficiency in the heat. Pre-menstrual symptoms in the late luteal phase can affect performance.
Menstruation, days 1 to 5 of the next cycle. Iron loss occurs. Some women experience fatigue and reduced performance during this phase, especially the first one or two days. Others are unaffected.
How much this matters varies enormously between individuals. Some women notice strong cycle-related performance differences. Others notice almost nothing.
What Patricia does, and what some research supports. Track your cycle. Notice patterns over 3 to 4 months. Schedule your hardest training sessions for the mid-follicular phase if possible. Pay extra attention to warm-up and avoid maximum-intensity lateral movements during the ovulatory window if you've had previous knee issues. Don't beat yourself up for lower performance during the late luteal phase or menstruation. It's biology, not lack of effort.
This is not prescription. This is information you can use to understand your own patterns.
The menstrual cycle has four rough phases. Each phase has different hormonal profiles that affect physiological function.
Follicular phase, roughly days 1 to 14. Estrogen rises gradually. Most research suggests this is when training adaptations happen most effectively. Energy levels and motivation tend to be higher in the mid-to-late follicular phase. Many female athletes report feeling strongest in this window.
Ovulation, around day 14. Peak estrogen. Joint laxity is highest. This is one of the higher-risk windows for ligament injuries. Some research suggests reducing maximum-intensity work around ovulation to reduce ACL risk.
Luteal phase, days 15 to 28. Progesterone rises. Core body temperature increases slightly. Some women experience reduced cardiovascular efficiency in the heat. Pre-menstrual symptoms in the late luteal phase can affect performance.
Menstruation, days 1 to 5 of the next cycle. Iron loss occurs. Some women experience fatigue and reduced performance during this phase, especially the first one or two days. Others are unaffected.
How much this matters varies enormously between individuals. Some women notice strong cycle-related performance differences. Others notice almost nothing.
What Patricia does, and what some research supports. Track your cycle. Notice patterns over 3 to 4 months. Schedule your hardest training sessions for the mid-follicular phase if possible. Pay extra attention to warm-up and avoid maximum-intensity lateral movements during the ovulatory window if you've had previous knee issues. Don't beat yourself up for lower performance during the late luteal phase or menstruation. It's biology, not lack of effort.
This is not prescription. This is information you can use to understand your own patterns.
Iron deficiency: the issue most amateurs miss
Iron deficiency is significantly more common in women athletes than in men. The combination of monthly menstrual blood loss, increased iron needs from athletic training, and often-restricted diets (women athletes are more likely to limit red meat) creates a real risk.
Symptoms can be subtle. Persistent fatigue that doesn't improve with rest. Reduced exercise tolerance. Difficulty recovering between sessions. Hair shedding. Brittle nails. Sometimes cold hands and feet. Sometimes nothing obvious until you collapse on the court.
EFSA confirms iron contributes to reduction of tiredness and fatigue, normal oxygen transport, and normal cognitive function.
What to do. If you've been tired for weeks and the usual fixes (sleep, food, hydration) aren't helping, get a blood test. Specifically ferritin (which reflects iron stores), hemoglobin, and a full iron panel. If your ferritin is below 30 ng per mL, you're at risk even if your hemoglobin is normal. Many sports physicians want female athletes' ferritin above 50.
Iron supplementation should be done under medical guidance. Too much iron is toxic. Self-supplementing without testing is not safe. But identifying low iron and correcting it can completely transform how you feel and perform.
Patricia got tested two years ago after months of unexplained fatigue. Her ferritin was 18. Three months of guided iron supplementation later, her energy was completely different. She told me she'd been operating at half capacity for years without realizing it.
Symptoms can be subtle. Persistent fatigue that doesn't improve with rest. Reduced exercise tolerance. Difficulty recovering between sessions. Hair shedding. Brittle nails. Sometimes cold hands and feet. Sometimes nothing obvious until you collapse on the court.
EFSA confirms iron contributes to reduction of tiredness and fatigue, normal oxygen transport, and normal cognitive function.
What to do. If you've been tired for weeks and the usual fixes (sleep, food, hydration) aren't helping, get a blood test. Specifically ferritin (which reflects iron stores), hemoglobin, and a full iron panel. If your ferritin is below 30 ng per mL, you're at risk even if your hemoglobin is normal. Many sports physicians want female athletes' ferritin above 50.
Iron supplementation should be done under medical guidance. Too much iron is toxic. Self-supplementing without testing is not safe. But identifying low iron and correcting it can completely transform how you feel and perform.
Patricia got tested two years ago after months of unexplained fatigue. Her ferritin was 18. Three months of guided iron supplementation later, her energy was completely different. She told me she'd been operating at half capacity for years without realizing it.
Pregnancy and padel: the questions I can't fully answer
This is medical territory and I'm going to be brief and direct.
The general guidance from sports medicine organizations is that women with uncomplicated pregnancies can continue moderate-intensity exercise throughout pregnancy, with modifications as the pregnancy progresses. This includes some racquet sports played at moderate intensity.
Padel specifically has not been studied much during pregnancy. The lateral movements, sudden changes of direction, and balance demands are factors that warrant individual medical assessment. Most obstetricians I've heard about through Patricia and other women players I've talked to are more comfortable with moderate padel during the first and second trimesters than with high-impact running.
Postpartum return to sport is highly individual. Pelvic floor recovery, abdominal recovery, breastfeeding considerations, sleep deprivation, time available. There's no single timeline.
What I can say with confidence. If you're pregnant or postpartum and want to play padel, this is a conversation with your obstetrician and a women's health physiotherapist who specializes in postpartum sport return. Not with the internet. Not with this article.
The general guidance from sports medicine organizations is that women with uncomplicated pregnancies can continue moderate-intensity exercise throughout pregnancy, with modifications as the pregnancy progresses. This includes some racquet sports played at moderate intensity.
Padel specifically has not been studied much during pregnancy. The lateral movements, sudden changes of direction, and balance demands are factors that warrant individual medical assessment. Most obstetricians I've heard about through Patricia and other women players I've talked to are more comfortable with moderate padel during the first and second trimesters than with high-impact running.
Postpartum return to sport is highly individual. Pelvic floor recovery, abdominal recovery, breastfeeding considerations, sleep deprivation, time available. There's no single timeline.
What I can say with confidence. If you're pregnant or postpartum and want to play padel, this is a conversation with your obstetrician and a women's health physiotherapist who specializes in postpartum sport return. Not with the internet. Not with this article.
Menopause and padel after 50
I touched on this in my padel after 40 article. Worth expanding here.
Perimenopause and menopause bring meaningful changes. Estrogen levels drop, which affects bone density, body composition, cardiovascular health, sleep quality, and joint comfort. Many women experience these changes between 45 and 55, sometimes earlier, sometimes later.
What can help for women who want to keep playing through these years.
Strength training becomes more important than ever. The loss of estrogen accelerates bone density decline. Mechanical loading from strength training is one of the best interventions for slowing this. Two to three sessions per week.
Calcium and vitamin D become more critical. EFSA confirms calcium contributes to maintenance of normal bones and vitamin D contributes to normal absorption of calcium and to maintenance of normal bones. Daily adequate intake matters.
Protein needs may be slightly higher. The combined effect of aging and hormonal change makes muscle maintenance harder. Higher protein intake (toward the 2 grams per kg body weight range) supports muscle synthesis.
Sleep disruption is common. Hot flashes affect sleep quality. Magnesium contributes to reduction of tiredness and fatigue (EFSA confirmed). Some women find magnesium helpful for sleep quality. Worth trying.
Joint comfort can change. The same training that worked at 45 may need adjustment at 55. More warm-up time. Less max-intensity work. More recovery between sessions.
I've watched women in their late fifties at my club continue playing strong padel. The ones doing well are the ones who adjusted their training, prioritized strength work, and stayed consistent through the transition years. The ones who tried to push through unchanged are the ones who got injured or quit.
Perimenopause and menopause bring meaningful changes. Estrogen levels drop, which affects bone density, body composition, cardiovascular health, sleep quality, and joint comfort. Many women experience these changes between 45 and 55, sometimes earlier, sometimes later.
What can help for women who want to keep playing through these years.
Strength training becomes more important than ever. The loss of estrogen accelerates bone density decline. Mechanical loading from strength training is one of the best interventions for slowing this. Two to three sessions per week.
Calcium and vitamin D become more critical. EFSA confirms calcium contributes to maintenance of normal bones and vitamin D contributes to normal absorption of calcium and to maintenance of normal bones. Daily adequate intake matters.
Protein needs may be slightly higher. The combined effect of aging and hormonal change makes muscle maintenance harder. Higher protein intake (toward the 2 grams per kg body weight range) supports muscle synthesis.
Sleep disruption is common. Hot flashes affect sleep quality. Magnesium contributes to reduction of tiredness and fatigue (EFSA confirmed). Some women find magnesium helpful for sleep quality. Worth trying.
Joint comfort can change. The same training that worked at 45 may need adjustment at 55. More warm-up time. Less max-intensity work. More recovery between sessions.
I've watched women in their late fifties at my club continue playing strong padel. The ones doing well are the ones who adjusted their training, prioritized strength work, and stayed consistent through the transition years. The ones who tried to push through unchanged are the ones who got injured or quit.
Equipment: what's actually different for women
Some equipment considerations that get mentioned in marketing aren't real differences. Others are.
Pala weight. Some manufacturers market women-specific pala lines that are simply lighter. The truth is that 350 grams or less is good for most amateurs regardless of sex. If you're a powerful player who wants more weight, get more weight. The women-specific label by itself means nothing.
Pala balance. Smaller hands often benefit from grip-balanced rather than head-balanced pales. This is more about hand size than sex but the correlation is significant.
Grip size. L1 is typical for smaller hands, L2 for medium, L3 for larger hands. Get the right size for your hand. Tennis-derived sizing standards work for padel.
Shoes. Women-specific padel shoes exist and are worth the slightly higher price for the better fit. The adoption gap I mentioned earlier shows women are already aware of this.
Clothing. Practical considerations only. Wear what's comfortable and lets you move. Skirts versus shorts versus leggings is personal preference, not a performance question.
Pala weight. Some manufacturers market women-specific pala lines that are simply lighter. The truth is that 350 grams or less is good for most amateurs regardless of sex. If you're a powerful player who wants more weight, get more weight. The women-specific label by itself means nothing.
Pala balance. Smaller hands often benefit from grip-balanced rather than head-balanced pales. This is more about hand size than sex but the correlation is significant.
Grip size. L1 is typical for smaller hands, L2 for medium, L3 for larger hands. Get the right size for your hand. Tennis-derived sizing standards work for padel.
Shoes. Women-specific padel shoes exist and are worth the slightly higher price for the better fit. The adoption gap I mentioned earlier shows women are already aware of this.
Clothing. Practical considerations only. Wear what's comfortable and lets you move. Skirts versus shorts versus leggings is personal preference, not a performance question.
Nutrition specifics worth mentioning
Most of my padel nutrition article applies to women players unchanged. A few specifics worth noting.
Iron, as covered above. Get tested if you're tired.
Calcium intake should be adequate, especially after 35. Dairy works. Fortified plant alternatives work. Leafy greens. Whatever fits your diet.
Folate matters during reproductive years, particularly if you're planning pregnancy. EFSA confirms folate contributes to normal psychological function and to maternal tissue growth during pregnancy.
Protein at every meal is important regardless of sex. Some research suggests women may benefit from slightly higher per-meal protein than the typical recommendations to maximize muscle protein synthesis. 30 to 40 grams per meal is a reasonable target.
Cycle-related cravings happen. Generally fine to honor them within reason. Forcing strict dietary discipline through PMS rarely improves anything.
Iron, as covered above. Get tested if you're tired.
Calcium intake should be adequate, especially after 35. Dairy works. Fortified plant alternatives work. Leafy greens. Whatever fits your diet.
Folate matters during reproductive years, particularly if you're planning pregnancy. EFSA confirms folate contributes to normal psychological function and to maternal tissue growth during pregnancy.
Protein at every meal is important regardless of sex. Some research suggests women may benefit from slightly higher per-meal protein than the typical recommendations to maximize muscle protein synthesis. 30 to 40 grams per meal is a reasonable target.
Cycle-related cravings happen. Generally fine to honor them within reason. Forcing strict dietary discipline through PMS rarely improves anything.
Where Rekova fits
This section is brief because I covered it more fully in my supplements article.
A daily recovery drink with proper electrolytes, magnesium, B vitamins, vitamin C, hydrolyzed collagen, and supporting nutrients covers many of the nutritional gaps that show up across the week.
For women players specifically, the iron consideration falls outside what daily supplements should address. Iron supplementation needs medical guidance and testing. We don't include iron in the Rekova formula for exactly this reason. Taking iron without testing your levels can cause real problems.
For everything else (the electrolytes, the magnesium for sleep and fatigue, the vitamin D, the collagen support, the B vitamins), the daily baseline matters. The convenience of one sachet versus eight bottles matters more for compliance over months.
I've recommended Rekova to Patricia and to a couple of other women players at my club. The feedback has been positive specifically around energy stability through the week and recovery between sessions.
A daily recovery drink with proper electrolytes, magnesium, B vitamins, vitamin C, hydrolyzed collagen, and supporting nutrients covers many of the nutritional gaps that show up across the week.
For women players specifically, the iron consideration falls outside what daily supplements should address. Iron supplementation needs medical guidance and testing. We don't include iron in the Rekova formula for exactly this reason. Taking iron without testing your levels can cause real problems.
For everything else (the electrolytes, the magnesium for sleep and fatigue, the vitamin D, the collagen support, the B vitamins), the daily baseline matters. The convenience of one sachet versus eight bottles matters more for compliance over months.
I've recommended Rekova to Patricia and to a couple of other women players at my club. The feedback has been positive specifically around energy stability through the week and recovery between sessions.
FAQ: questions women players ask
Do I really need different supplements as a woman? Iron is the main one to be aware of. Magnesium, vitamin D, B vitamins, electrolytes are needed by all athletes. The dosing isn't dramatically different.
Should I play during my period? Up to you. Some women feel fine playing throughout their cycle. Others have a day or two where they prefer to skip. There's no medical reason to avoid play unless you have specific gynecological conditions that make it uncomfortable.
When should I get my iron tested? If you've been unusually tired for more than 3 weeks despite adequate sleep, get tested. If you're vegetarian or vegan or limit red meat, get tested annually. If you're pregnant or postpartum, your doctor will test.
Can I play padel during pregnancy? Maybe. Talk to your obstetrician. Most uncomplicated pregnancies allow moderate exercise into the second trimester. Padel specifically depends on your individual situation.
How do I find a women's specific physiotherapist? Search for women's health physiotherapy or pelvic floor physiotherapy in your area. They handle postpartum return to sport and other female-specific issues.
Is there a difference in technique between men's and women's padel? Less than people think. The fundamentals are the same. Women may benefit slightly more from emphasizing positioning and shot selection given typically lower power compared to male opponents. But this is a generalization with many exceptions.
Do women progress at padel slower than men? In raw athletic terms, slightly. In actual game ability, no. The sport rewards positioning, anticipation, and shot selection at least as much as power. Plenty of women players at my club are technically stronger than the muscular men they regularly beat.
Is mixed doubles different from women's doubles? Tactically yes. The power differential between male and female players in mixed doubles changes shot selection and positioning. Women's doubles tends to feature more sustained rallies and stronger emphasis on placement. Different game, similar fundamentals.
Should I play during my period? Up to you. Some women feel fine playing throughout their cycle. Others have a day or two where they prefer to skip. There's no medical reason to avoid play unless you have specific gynecological conditions that make it uncomfortable.
When should I get my iron tested? If you've been unusually tired for more than 3 weeks despite adequate sleep, get tested. If you're vegetarian or vegan or limit red meat, get tested annually. If you're pregnant or postpartum, your doctor will test.
Can I play padel during pregnancy? Maybe. Talk to your obstetrician. Most uncomplicated pregnancies allow moderate exercise into the second trimester. Padel specifically depends on your individual situation.
How do I find a women's specific physiotherapist? Search for women's health physiotherapy or pelvic floor physiotherapy in your area. They handle postpartum return to sport and other female-specific issues.
Is there a difference in technique between men's and women's padel? Less than people think. The fundamentals are the same. Women may benefit slightly more from emphasizing positioning and shot selection given typically lower power compared to male opponents. But this is a generalization with many exceptions.
Do women progress at padel slower than men? In raw athletic terms, slightly. In actual game ability, no. The sport rewards positioning, anticipation, and shot selection at least as much as power. Plenty of women players at my club are technically stronger than the muscular men they regularly beat.
Is mixed doubles different from women's doubles? Tactically yes. The power differential between male and female players in mixed doubles changes shot selection and positioning. Women's doubles tends to feature more sustained rallies and stronger emphasis on placement. Different game, similar fundamentals.
The short version
Most padel research uses male subjects. Most of what works applies regardless of sex. The genuine differences worth knowing about are body composition, joint structure (especially knee and ACL), menstrual cycle effects, iron metabolism, bone density trajectory, and pregnancy and menopause transitions. Women face higher rates of ankle and knee injuries, particularly ACL tears. Iron deficiency is much more common and underdiagnosed. The fundamentals of sleep, training, nutrition, and recovery work the same way for women as for men, just sometimes need slight adjustments. Most women-specific marketing in sports equipment and supplements is exactly that, marketing. The genuine considerations are medical and physiological, and worth understanding for any woman playing regularly.
Sources
Smith Palacio E. Epidemiologia de las lesiones en padel y recomendaciones preventivas. Ciencia y Deporte. April 2024.
Dahmen J. et al. Incidence, prevalence and nature of injuries in padel: a systematic review. BMJ Open Sport and Exercise Medicine. 2023.
McNulty KL et al. The effects of menstrual cycle phase on exercise performance in eumenorrheic women: a systematic review and meta-analysis. Sports Medicine. 2020.
International Olympic Committee. Consensus statement on the female athlete triad and relative energy deficiency in sport. British Journal of Sports Medicine. 2023.
EFSA. Scientific Opinions on the substantiation of health claims related to iron, calcium, vitamin D, magnesium, and folate. EFSA Journal, various years.
Healthspan Elite. Padel: what is it and how should you fuel your game? Knowledge Hub. 2025.
Padel Magazine. Women in padel: training and equipment considerations. 2024.
ACSM. Position stand on physical activity and bone health. 2024.
American College of Obstetricians and Gynecologists. Physical Activity and Exercise During Pregnancy and the Postpartum Period. 2024.
This article shares research-based observations and conversations with female padel players, including Patricia. It is not medical advice and is not a substitute for individualized medical guidance, particularly for issues related to pregnancy, postpartum recovery, menopause, or specific medical conditions. If you have any concerns about your health, hormonal changes, or athletic performance as a woman, please consult a qualified healthcare professional with experience in women's sports medicine.
Rekova does not treat any medical condition and is not a substitute for medical care. It is a daily functional drink with electrolytes, magnesium, hydrolyzed collagen, B vitamins, vitamin C, CoQ10, Acetyl-L-Carnitine, and supporting nutrients, formulated as nutritional support for people who play padel regularly. The formula does not include iron, which requires individualized medical guidance.
Dahmen J. et al. Incidence, prevalence and nature of injuries in padel: a systematic review. BMJ Open Sport and Exercise Medicine. 2023.
McNulty KL et al. The effects of menstrual cycle phase on exercise performance in eumenorrheic women: a systematic review and meta-analysis. Sports Medicine. 2020.
International Olympic Committee. Consensus statement on the female athlete triad and relative energy deficiency in sport. British Journal of Sports Medicine. 2023.
EFSA. Scientific Opinions on the substantiation of health claims related to iron, calcium, vitamin D, magnesium, and folate. EFSA Journal, various years.
Healthspan Elite. Padel: what is it and how should you fuel your game? Knowledge Hub. 2025.
Padel Magazine. Women in padel: training and equipment considerations. 2024.
ACSM. Position stand on physical activity and bone health. 2024.
American College of Obstetricians and Gynecologists. Physical Activity and Exercise During Pregnancy and the Postpartum Period. 2024.
This article shares research-based observations and conversations with female padel players, including Patricia. It is not medical advice and is not a substitute for individualized medical guidance, particularly for issues related to pregnancy, postpartum recovery, menopause, or specific medical conditions. If you have any concerns about your health, hormonal changes, or athletic performance as a woman, please consult a qualified healthcare professional with experience in women's sports medicine.
Rekova does not treat any medical condition and is not a substitute for medical care. It is a daily functional drink with electrolytes, magnesium, hydrolyzed collagen, B vitamins, vitamin C, CoQ10, Acetyl-L-Carnitine, and supporting nutrients, formulated as nutritional support for people who play padel regularly. The formula does not include iron, which requires individualized medical guidance.
